- Group home
- You must register/login in order to post into this group.
Introducing recycling into the operating theatres
By: Oxford University Hospitals NHS Trust
Diversion of waste from landfill and incineration to recycling, saving money and carbon; engaged and empowered theatre staff across the OUH Trust in a successful change management project.
£1319.38 (NB this is a partial result, based on only 1 out of the 3 participating theatre suites) (Estimated)
8,886 kg CO2e (NB this is a partial result, based on only 1 out of the 3 participating theatre suites) (Estimated)
The Oxford University Hospitals Trust has reduced the amount of waste going to landfill or incineration by introducing recycling into the operating theatre setting. Previously all waste from clinical areas was disposed of via orange clinical waste bags. There are now recycling bins in every anaesthetic room of the three largest operating suites, as well as in recovery and staff rest areas. Waste segregation has become routine for many members of staff and approximately 22% of theatre waste is now recycled.
DOWNLOAD CASE STUDY AS PDF HERE.
Implementation
1. Engaging colleagues / changing behaviour
The project was initiated by an anaesthetic trainee and operating department practitioners (ODPs) working together. To engage colleagues, they began by presenting a survey about recycling to ALL staff working in the three largest operating suites in the Trust. The aims of this survey were to:
- Survey current waste segregation behaviour at home and work
- Highlight the differences in behaviour between home and work
- Identify barriers to recycling at work
The survey therefore acted both as a tool for data collection and an intervention. Results showed that while 96% of staff recycle at home, only 60% do so at work - and to a lesser extent.
Next, they observed workflows to identify the main disposers of physical waste in theatres. These key groups were subsequently targeted for education at clinical governance days:
- anaesthetic nurses
- operating department practitioners (ODPs)
- circulating/scrub nurses
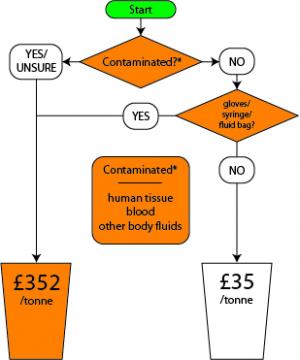
A flow chart algorithm was placed by each of the new recycling bins as an aide memoire.
2. Infrastructure
In October 2011, 70 corrugated plastic recycling bins were purchased and were placed in every anaesthetic room, and in recovery and staff rest areas of the three largest operating suites. Funding for the first 20 bins came from one of the Operating Department budgets, with subsequent bins paid for by Estates.
3. Measuring impact
In February 2012, four months after introduction of the new bins, the extent of recycling was assessed via a one-day waste audit conducted in the John Radcliffe (JR) main theatre suite.
On the day of data collection theatre orderlies were asked to leave all waste in a certain place so that it could be counted prior to placing in the large wheelie bins. At regular intervals throughout the day the bags were counted and the numbers of orange clinical waste bags and clear recycling bags were recorded. Black bin bags for domestic waste are only provided in recovery and staff rest areas (not in anaesthetic rooms or operating rooms), and these were not recorded. There were nine theatre lists running, and data was collected from 8am to 6pm during which time most (but not all) of the elective lists had finished operating. In total there were 31 orange and 18 clear waste bags.
The average weight of an orange clinical waste bag was calculated by weighing 20 bags. Similarly, the average weight of a clear recycling bag was calculated from 10 bags:
- Orange clinical waste bag = 1.785kg
- Clear recycling bag = 0.87kg
Total waste produced on day of collection*:
- Clinical waste = 31 bags x 1.785kg = 55.335kg (78%)
- Recycled waste = 18 bags x 0.87kg = 15.66kg (22%)
*NB - this is likely an underestimate as some theatres would not have finished operating and deposited their waste by 6pm
Cost savings
The main JR theatres run an average of 46 lists per week, which equates to 2392 lists per year. On the day of data collection there were nine lists running, so an average weight of the waste produced per list could be calculated:
- Clinical waste/list = 55.335/9 = 6.15kg/list
- Recycled waste/list = 15.66/9 = 1.74kg/list
By multiplying by 2392 an approximate value for the amount of clinical waste produced per year can be obtained:
- Clinical waste per year = 6.15 x 2392 = 14706.81kg = 14.70681 tonnes
- Recycled waste per year = 1.74 x 2392 = 4162.08kg = 4.16208 tonnes
Disposing of clinical waste costs £352 per tonne, compared with £35 per tonne for mixed recycling. Assuming that all waste that is currently recycled would previously have been disposed of as clinical waste, the financial savings over a year can be estimated:
- Previous cost of disposing clear bag waste (as clinical waste), per year = 4.16208 x £352 = £1465.05216
- Current cost (as recycled waste), per year = 4.16208 x 35 = £145.6728
Cost saving = £1319.38 per year
Carbon Savings:
Greenhouse gas (GHG) conversion factors for waste disposal were obtained from the 2011 Guidelines to Defra / DECC's GHG Conversion Factors for Company Reporting (Table 9d).
The GHG for incineration of clinical waste was taken as 1,833 kg CO2e emitted per tonne of waste (DEFRA emissions factors for incineration do not specifically account for clinical waste, which is commonly undertaken at higher temperatures. To reflect the increased emissions that are likely to result from the incineration of clinical waste, the highest available emissions factor for incineration was applied).
The GHG for recycling of waste was taken as -302 kg CO2e / tonne. This is based on conversion factors for paper (-157 kg CO2e / tonne) and plastic film (-447 kg CO2e). We assumed a composition by weight of 50% paper and 50% plastic to produce a combined conversion factor of -302.
Using these factors we estimated the GHG savings per year:
- Previous GHG emissions from disposing clear bag waste (as clinical waste), per year = 4.16208 tonnes x 1833 kg CO2e per tonne = 7,629 kg CO2e
- Current GHG (as recycled waste), per year = 4.16208 x -302 kg CO2e per tonne = -1,257 kg CO2e
Saving = 8,886 kg CO2e per year
Acknowledgement: Thanks to final year medical student Felicity Hughes for her assistance in conducting the waste audit and drafting this case study.
Main Operating Theatre Suite and West Wing Theatre Suite, John Radcliffe Hospital; Operating Theatres, Churchill Hospital
The primary aim of the project was to reduce the carbon footprint of theatres whilst proving that the Trust could save money with minimal financial investment. The secondary aim was to encourage staff to challenge their own working practices using the paradigm of “reduce, reuse, recycle”. Whilst recycling of physical waste offers a relatively easy initial target, it is hoped that this project will lead to more ambitious ones, e.g. novel equipment and drug stock management (“reduce”), carbon footprinting care pathways (“reduce”).
- Embed waste segregating behaviour in the operating theatres.
- Introduce competition between operating suites.
01/02/2011
ongoing
£700 (cost of bins across all three theatre suites)
Recycling questionnaire obtained from the Green Nephrology Network at http://sustainablehealthcare.org.uk/green-nephrology/resources/2012/03/staff-recycling-questionnaire
Dr Mark Scarfe, Specialist trainee in anaesthetics, mscarfe@doctors.org.uk